
Robotic assisted simple prostatectomy (RASP)
What is involved in the RASP procedure?
Your prostate gland surrounds your urethra as it exits the bladder. When it enlarges (BPH), it can obstruct the urine flow. In the cases of very large glands (>120 cc), the standard transurethral approaches are inadequate and at times unsafe. A simple prostatectomy is performed to address an enlarged prostate. If you envision the prostate as an orange, the objective of this procedure is to extract the flesh while leaving the rind intact. Since the complete removal of the prostate is not undertaken, the associated risks of erectile dysfunction and urinary incontinence are minimal.
This surgery involves the removal of the obstructing central portion of the prostate gland through a minimlay invasive keyhole procedure using the robotic platform. It is specifically employed when the prostate is excessively large or unsuitable for removal using a telescope.
Our goals in men with a significantly obstructing prostate gland include:
Removing the obstructing lobes.
Facilitating a stronger urine flow.
Alleviating as many urinary symptoms as possible.
Preserving continence.
Safeguarding the nerves responsible for erection to the penis.
At the conclusion of the operation, it is customary to insert a temporary bladder catheter and left in place for r days. The open simple prostatectomy has been the established standard of care for addressing large prostate glands over many years. The robotic approach replicates this procedure while offering the added advantage of being minimally invasive and substantially reducing blood loss. A/Prof Zargar has been actively engaged in this procedure for over a decade and has contributed extensively to significant international publications evaluating the safety and efficacy of this approach.A/Prof Homi Zargar, performs this procedure at Melbourne western suburbs (Western private hospital) and at Epworth, Richmond.

RASP main points
Key Points:
Robotic Simple Prostatectomy (RASP)
RASP is a surgical procedure designed to eliminate the central obstructing lobes of the prostate while preserving the outer shell and capsule.
This procedure offers enhanced precision and dexterity, conducted with a robot, contributing to a more refined and minimally invasive approach.
The operation concludes with placing a catheter, which remains in place for six days.
This procedure is reserved for large prostate glands.
A/Prof H.Zargar can assess whether the size and shape of your prostate make you a suitable candidate for this procedure. However, it may not be suitable for all men with prostate enlargement. Very large prostate glands are not suitable for TURP.
surgery
What occurs on the day of the procedure?
A/Prof Homi Zargar will discuss the surgery once again to ensure your understanding and obtain your consent. An anesthetist will meet with you to explore the options of a general or spinal anesthetic and discuss post-procedure pain relief.
Details of the procedure:
The procedure is performed under general anesthesia, ensuring the patient is asleep.
All methods aim to minimize postoperative pain.
Prior to the procedure, an antibiotic injection is administered after thorough allergy checks.
The abdominal cavity is inflated with carbon dioxide gas to facilitate the operation.
Typically, six keyhole incisions are made in the abdomen, allowing for the insertion of surgical instruments.
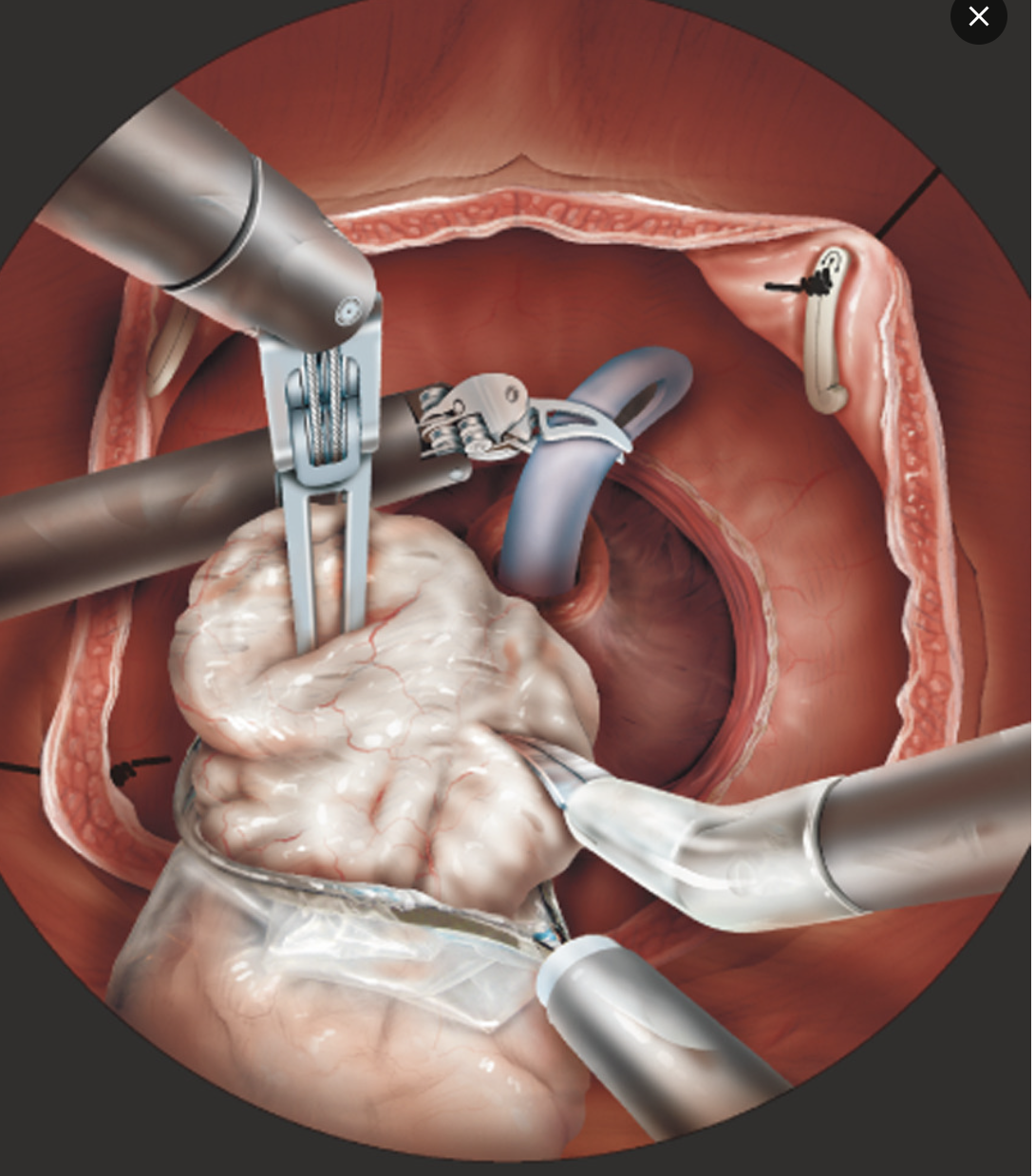
A small incision in the bladder provides access to the interior of the prostate, which is then removed, leaving the outer capsule intact.
A sample of prostate tissue is sent to the laboratory for analysis.
The bladder is closed, and a catheter is placed through the urethra to drain urine until the join heals.
The incisions are closed with dissolvable stitches or staples.
A drain (a plastic tube from the abdomen) may be present for a few days post-surgery.
The catheter usually remains in place during the hospital stay and is removed in 6 days .

After-Effects and Risks of the Procedure:
No semen production during orgasm, resulting in effective infertility for all patients.
Almost all patients experience persisting symptoms of urgency and frequency by day, along with nocturnal urination.
Inability to pass urine after catheter removal, requiring intermittent catheterization or a permanent catheter, occurs in 3 to 5% of patients.
Erectile dysfunction (impotence) may occur in 1 in 10 to 1 in 50 patients.
The intact outer layer of the prostate poses a potential risk of developing future prostate cancer; discussions about PSA testing with the surgeon and GP are recommended for 1 in 10 to 1 in 50 patients.
Pathology tests may reveal unexpected cancer in the removed prostate tissue, requiring observation, investigations, and/or possible further treatment, affecting 1 in 10 to 1 in 50 patients.
Bleeding requiring transfusion or further surgery is extremely rare with robotic approach (1 in 50 to 1in patients 250).
Scarring of the bladder neck or urethra, requiring stretching or further treatment, is rare with robotic approach(1 in 50 to 1in patients 250).
Pain, infection, or hernia in the incision, requiring additional treatment, affects 1 in 50 patients.
Possible anaesthetic or cardiovascular problems that might necessitate intensive care admission occur in 1 in 50 to 1 in 250 patients. Individual risk estimates can be provided by the anaesthetist.
Temporary urinary incontinence requiring pads may affect 1 in 50 to 1 in 250 patients. If it persists for more than a year, further surgery may be required, involving an artificial urinary sphincter or a synthetic male sling.